





What is viral Hepatitis?
Viral hepatitis is an infection that involves predominantly the liver. As of today, five unrelated hepatotropic pathogens, hepatitis A virus (HAV), hepatitis B virus (HBV), hepatitis C virus (HCV), hepatitis D virus (HDV), and hepatitis E virus (HEV) are recognized to cause almost all cases of viral hepatitis. Viral hepatitis is a global health problem. Hepatitis viruses play a significant role in the story of global disease and death and pose a colossal health challenge and despair.
What causes Hepatitis A?
Hepatitis A is an infection of the liver etiologically related to HAV. Hepatitis A has global distribution with endemicity proportional to socio-economic conditions and standards of sanitation and hygiene. HAV infection is predominantly spread from one person to another through the orofecal route or by contaminated food and water. The clinical outcome is strongly correlated with age, being mostly subclinical ≤6 years and symptomatic in older children and adults.
What about the Hepatitis A virus?
HAV is an RNA virus, classified in the hepatovirus genus of the Picornaviridae family. HAV exists only as a single serotype, with three genotypes (1-III) that circulate in humans and three additional genotypes (IV-VI) recognized in non-human primates. Humans are the only natural host for HAV. The virus is a heat-stable and acid/ether-resistant RNA virus. The virion is a non-enveloped, symmetrical, small 27-nm, spherical particle. The HAV genome is about 7.5 kb (Fig 1).
What about global Hepatitis A epidemiology?
The epidemiology of hepatitis A is based on population-based seroprevalence (IgG anti-HAV) studies. The world is divided into 3 zones. The very high endemic zone includes resource-poor countries with poor sanitary conditions, overcrowding, contaminated water, and food which promotes universal exposure to HAV infection in children soon after weaning. The majority of these infections are subclinical and seroconversion is usually asymptomatic.
HAV infection in adults is rare and outbreaks of HAV infection are rare in such countries. High-to-intermediate endemic zone exists in developing countries where there is recent continued improvement in sanitary conditions and access to safe water and reduced exposure of children to HAV infection.
Such regions of the World have a high occurrence of clinical hepatitis A in young adults. Low endemic zone of HAV spreads over the developed world and exposure to children in these countries is infrequent and anti-HAV seropositivity increases slowly throughout early childhood. Outbreaks and large-scale epidemics of HAV have been traced to contaminated foods and fruits, imported from endemic zones.
How does it spread?
There are two main ways hepatitis A spreads namely through the person-to-person spread and contaminated food and water. Humans are the lone hosts and source of spread and transmission for HAV and there are no animal sources for the spread of the disease. HAV infection is spread directly from one person to another through the orofecal route.
Large quantities of the virus are shed in feces from the late incubation period until the first week of clinical disease. The infectious period starts 1 to 3 weeks before and lasts for 1 to 8 days after the onset of jaundice. The transmission is supported by low hygiene, overcrowded families, and close contact.
Contaminated food and water can transmit HAV infection. Foods of diverse natures like milk, milk products, seafood, salads, and ice creams can get contaminated. Infected food handlers may contaminate foodstuffs and beverages and result in outbreaks of HAV. HAV can spread rarely through blood transfusion, IV drug use, and through sex among men having sex with men or oral sex.
What about Hepatitis A disease?
Acute hepatitis A presentation resembles a disease caused by other hepatitis viruses and may vary from mild short-lasting icteric disease to acute liver failure. Hepatitis A causes acute hepatitis which is self-limiting and does not cause chronic infection. The clinical outcome is strongly correlated with age. HAV infection in children below 6 years of age is either asymptomatic or subclinical; while older children and adults commonly experience symptomatic disease.
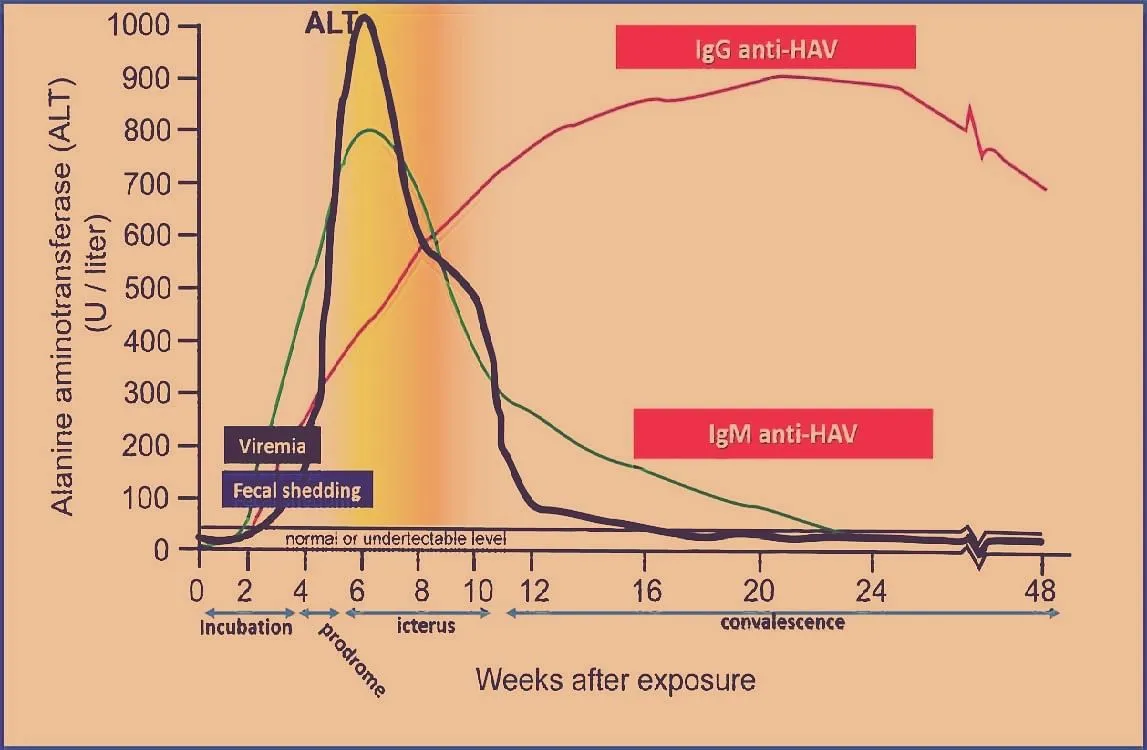
Acute hepatitis A disease passes through four phases including the incubation period (15-45 days), prodromal symptoms (1-7 days), icteric period (2-6 weeks), and convalescence (up to 6 weeks) (Fig 2).
During the incubation period, the patient is asymptomatic but is infectious. Patients develop constitutional symptoms which include low-grade fever, anorexia, nausea and vomiting, abdominal discomfort, diarrhea, fatigue, malaise, arthralgia, myalgia, and headache.
The icteric phase starts with dark urine and light-colored stools and within 1-5 days’ patients develop icterus of sclera and skin. With the appearance of jaundice, there is a significant abatement of systemic symptoms. Physical examination reveals icterus and tender hepatomegaly.
Clinical examination is unremarkable except for mild tender hepatomegaly. Complete clinical and biochemical recovery occurs in all patients. A small percentage may present with an unusual variant called cholestatic hepatitis A which lasts for 12 to 18 weeks.
Fulminant hepatitis A occurs in 1:1000 cases of acute hepatitis A and may be fatal. The disease can be recognized early on by worsening prothrombin time, a significant reduction in liver size (detected on percussion for liver dullness), irritability, and alteration in sleep rhythm. The risk for the fulminant disease increases with patients’ age and is particularly high in patients above 30 years.
How to diagnose Hepatitis A?
Acute hepatitis caused by HAV is diagnosed by liver function tests. Serum bilirubin rises above 2.5 mg/dl during the icteric phase of the disease. Serum bilirubin rises to levels ranging from 5-20 mg/dl. Hyperbilirubinemia is biphasic, with the rise of both conjugated and unconjugated bilirubin. Deep jaundice with serum bilirubin levels of 20 mg/dl is associated with severe disease.
Alanine transaminase (ALT) and aspartate transaminase (AST) are elevated during the prodromal phase and can reach 400-4000 IU or more. Serum alkaline phosphatase may be normal or show mild elevation. However, patients with cholestatic hepatitis A depict marked elevation of serum alkaline phosphatase. Prothrombin time has prognostic significance and prolonged values occur in patients with severe hepatic synthetic defect, which signifies extensive hepatocellular necrosis.
Diagnosis of HAV is made by determining IgM antibody to HAV (IgM anti-HAV) and is the gold standard for diagnosis of acute HAV infection. Looking for HEV RNA is not needed and is rarely employed for the diagnosis of acute hepatitis A.
How to treat Hepatitis A?
Patients with acute hepatitis A need supportive treatment. No specific antiviral therapy is available. During the prodromal period, nausea and vomiting need treatment with an antiemetic. Few patients require a short hospital stay to manage dehydration. Intravenous alimentation is rarely needed in patients who have persistent vomiting and cannot maintain oral intake. Patients often need bed rest with bathroom privileges during prodromal and icteric disease.
Later patients should be advised to restrict activity and no-work advice till disease recovery ensues. Restriction of diet has no proven benefit. A high-calorie diet is advisable. A low-fat, high-carbohydrate diet is often enforced. However, apart from being palatable, this regimen has no added advantage.
Alcohol and hepatotoxic drugs should be avoided. Acetaminophen may be administered if needed to a maximum dose of 2-4 g/day in adults. Patients with cholestasis benefit from bile salt sequestering resin cholestyramine and/or ursodeoxycholic acid (UDCA). Corticosteroid therapy has no role, even in severe cases.
At the outset, it is not possible to predict the course of the disease and all patients need to be watched carefully for severe disease and impending acute liver failure. Patients with rapidly shrinking liver size, high INR, a rapid rise in serum bilirubin, and ascites with confusion, altered sleep pattern, and disorientation should be identified early and admitted to intensive care for the management of acute liver failure. Liver transplantation has been done in patients with progressive liver failure.
What is the role of Hepatitis A vaccine?
Both passive and active immunization are playing a major role in the control of hepatitis A. Immune serum globulin (Ig) 0.02 ml/kg should be administered intramuscularly to intimate contacts and prevents clinical disease in those who have been exposed to the virus.
Several HAV vaccines are available. HAV vaccine is safe, immunogenic, and effective in preventing hepatitis A. Vaccine is safe above 1 year of age and protects 4 weeks after primary inoculation. HAV vaccination programs are not recommended in very high-endemic areas.
In such countries, there is universal exposure to HAV infection in children below 5 years of age and the population is protected from HAV infection. However, the HAV vaccine has been successfully used to control community-wide outbreaks. Vaccination should be initiated early on during the epidemic. Supplemental health education and improved sanitation need to be enforced.
How to control Hepatitis A?
The control of hepatitis A is dependent upon improved socio-economic status and improvement in living standards, which in turn reduce virus transmission in the community and disease burden, independent of other measures.
Another important measure is to supply safe potable drinking water and ensure proper sewage disposal to reduce person-to-person transmission of HAV infection. We need to target personal hygiene practices like regular hand washing, especially in schools, offices, and homes for the mentally challenged, etc. which helps to reduce the risk of infection. Western tourists should be discouraged from ingestion of uncooked or inadequately cooked foods, salads, untreated tap water, and ice creams.
(Prof. Mohammad Sultan Khuroo is MD, DM, FRCP (Edin), FACP, Master American College of Physicians (MACP, Emeritus) and former Director, Professor and Head Gastroenterology, Chairman Dept. Medicine, Sher-I-Kashmir Institute of Medical Sciences, Soura, Srinagar, Kashmir, India.Director, Digestive Diseases Centre, Dr.Khuroo’s Medical Clinic, Srinagar, Kashmir, India. The author can be mailed khuroo@yahoo.com, mohammad.khuroo@gmail.com, Website: www.drkhuroo.com.)
DISCLAIMER: The views and opinions expressed in this article are the personal opinions of the author.
The facts, analysis, assumptions and perspective appearing in the article do not reflect the views of GK.